

SAN DIEGO — Research presentations, based on the current literature of prehospital trauma care, were a highlight at the National Association of EMS Physicians annual meeting. Here are quick summaries and key takeaways from the papers that were presented involving EMS trauma care.
Bleeding control: hemostatic bandages
Hemostatic bandages received a weak recommendation from ILCOR for their ability to stop external bleeding when direct pressure fails, or the application of a tourniquet is not possible. This recommendation is because the research done on the efficacy of hemostatic bandages is not especially strong. However, it was felt that there was good rationale for use of hemostatic bandages for bleeding control in civilian EMS.
Bleeding control: tourniquets
Similarly, tourniquet use also received a weak ILCOR recommendation because of the relative weakness of the studies conducted on their use. Many of the studies were conducted in military arenas and not in civilian trauma care.
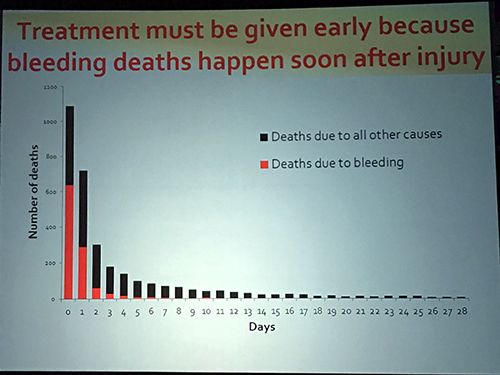
A slide from the National Association of EMS Physicians presentation. (Photo by Arthur Hsieh)
Permissive hypotension
Researchers reported that controlled resuscitation, also known as permissive hypotension, appears to increase the survival rate of trauma patients who are in shock. Systolic blood pressures, as low 70 mm Hg, are well tolerated and may benefit long-term patient survival.
Optimal systolic blood press
On the opposite spectrum, there may be an optimal systolic blood pressure range for brain injured patients. That optimal systolic pressure may be much higher than previously thought to be acceptable. Current teaching in brain injury management is to support a patient blood pressure at 90 mm Hg systolic or higher. Research has indicated that an optimal systolic blood pressure may range between 130 to 192 mm Hg.
TXA administration for internal hemorrhage
The administration of transexamic acid to patients with traumatic internal bleeding appears to improve survival. In addition, several studies indicate that early TXA use, less than an hour after the initial traumatic insult, produces the greatest positive effect, reducing the patient mortality rate by a third. Conversely, administering TXA more than 3 hours after the traumatic injury was potentially harmful to the patient.